Skip to content
Angle Recession
- Separation between the longitudinal and circular muscle of the ciliary body (commonly caused by blunt injury to the eye)
- Incidence of intraocular pressure elevation appears to be directly related to the extent of angle involvement (may require at least 180 or 270 degree involvement)
Clinical Features
- Symptoms:
- May be asymptomatic
- In the acute phase following injury, early onset glaucoma may be related to concurrent uveitis or hyphema
- Signs:
- Intraocular pressure may remain normal for years or decades before becoming elevated
- Associated findings may include corneal edema, pupillary sphincter tear, subluxated lens, or hyphema
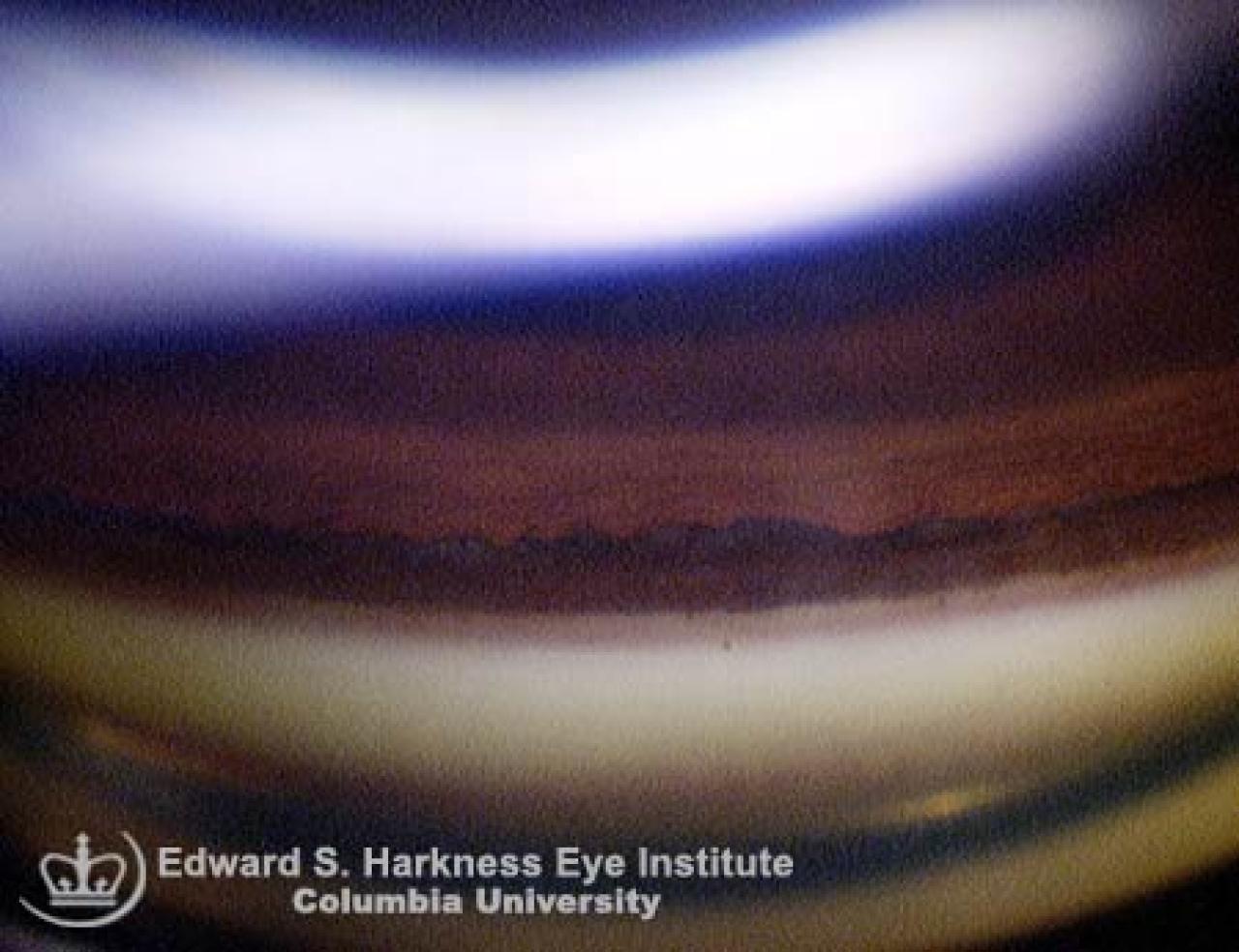
- Gonioscopic examination may demonstrate:
- The classic finding of a widened ciliary body band
- Posterior iris displacement
- Baring of the ciliary processes
Management
- Routine follow-up of patient with recessed angle but no IOP elevation
- Topical steroid therapy may be used with early post-traumatic IOP elevation believed secondary to increased outflow resistance from trabecular edema and inflammation
- Anti-glaucoma medications such as aqueous suppressants (e.g. beta adrenergic antagonists), alpha2 adrenergic agonist, and miotics may be given
- Surgical treatment (e.g. glaucoma filtration surgery) may be indicated for glaucoma unresponsive to medical therapy
Back to top