Skip to content
Serpiginous Choroiditis
- Rare, chronic, bilateral inflammatory disorder
- Recurrences are common
- Onset is usually between ages 30 and 70 years
Clinical Features
- Symptoms:
- Painless blurring of vision with central or paracentral scotoma
- Metamorphopsia due to macular involvement
- Signs:
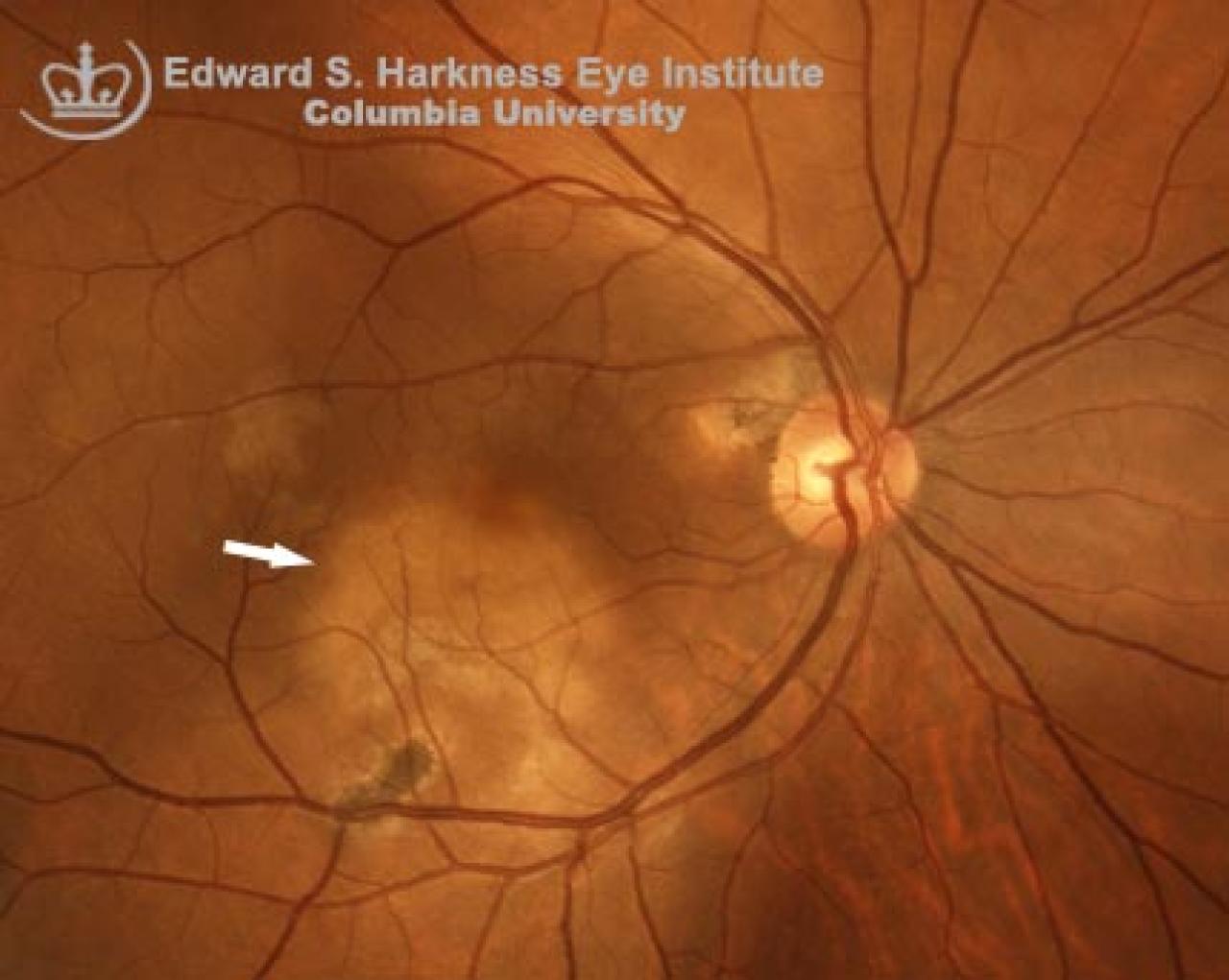
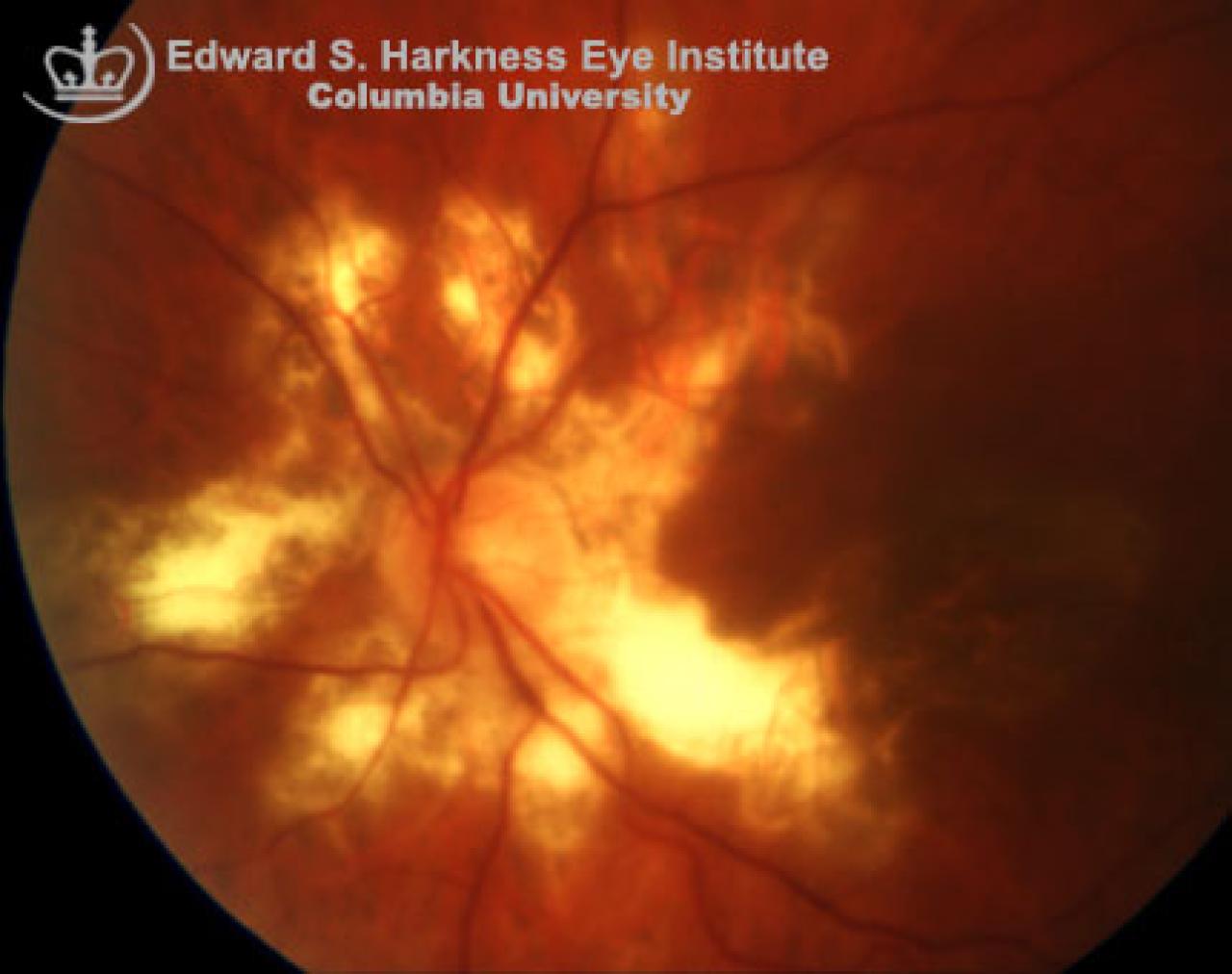
- Acute onset lesion: gray-yellowish discoloration of the RPE with a pseudopodial configuration extending in a centrifugal manner from the optic disc
- Acute lesions normally last in several weeks, followed with development of chorioretinal atrophy and RPE migration along the large choroidal vasculature
- Previous inflammation is evidence with areas of atrophic RPE, choriocapillaris and pigment clumpings
- New lesions are often contiguous with the chronic lesions
- Can be complicated with choroidal neovascularization
Fluorescein Angiogram Demonstrates
- Acute lesions: hypofluorescence in the early phases and hyperfluorescence with leakage or staining of the lesion evolving centrally in the mid to late phases
- Mottled hyperfluorescence due to pigment clumping in chronic lesions
- Electrophysiologic studies are normal.
- Occasional cases have been associated with the administration of anti-tuberculosis drugs.
Management
- Self assessment with Amsler grid test
- Triple immunosuppression with; systemic corticosteroid, acyclovir and cyclosporin in vision threatening cases, such as macular or papillomacular involvement.
- Laser photocoagulation and submacular surgery in cases complicated with choroidal neovascularization.
Back to top