X-linked Juvenile Retinoschisis
- Affects only males
- Female carriers have normal vision and are normal on ophthalmic examination
- Age of onset is in the first decade
- Histopathologically, there is a split between the nerve fiber and ganglion cell layer
Clinical Features
- Symptoms: decreased central vision (20/25 - 20/50) and slowly progressive
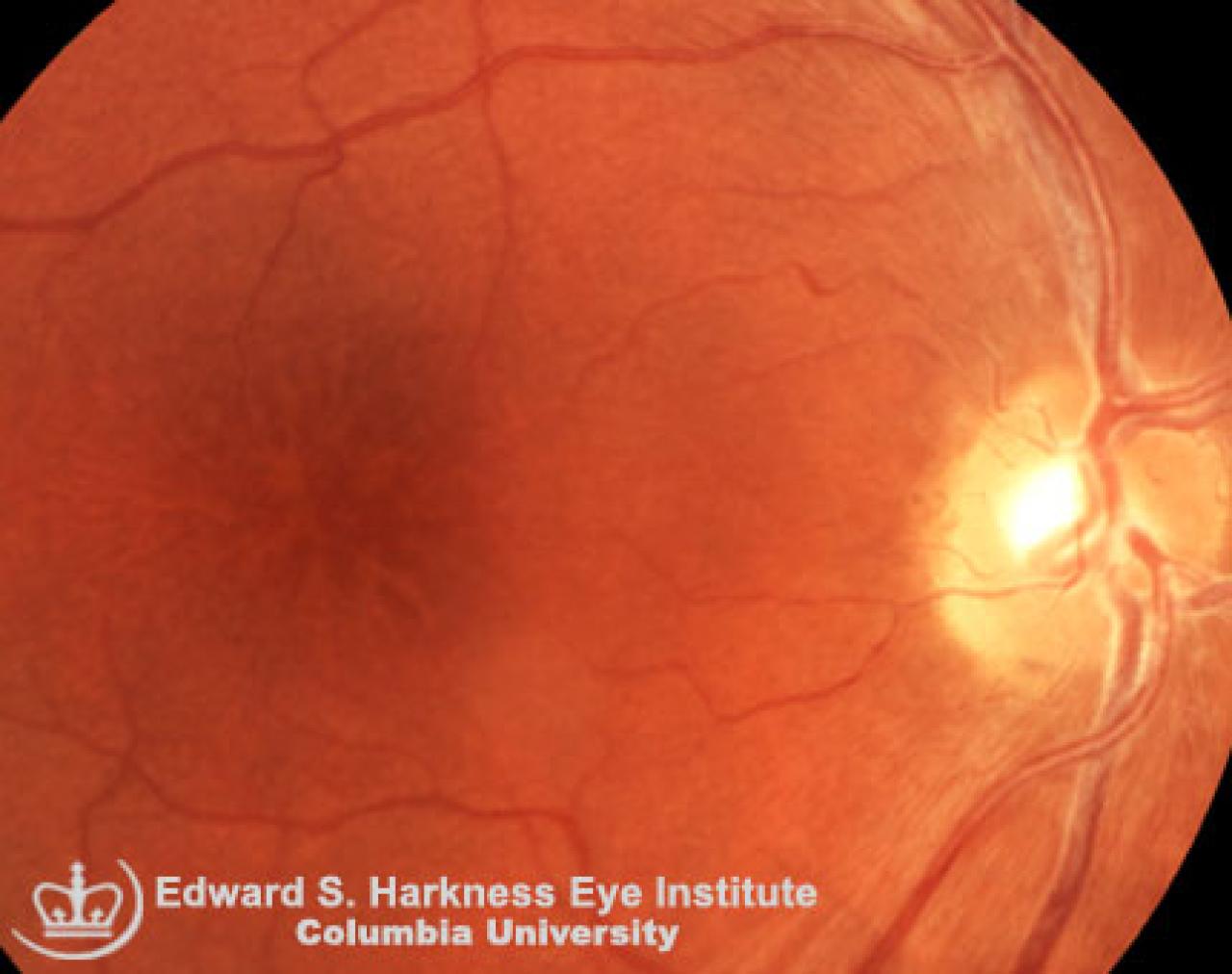
- Signs:
- Presence of perifoveal microcystic changes with spoke wheel-like plications of the overlying ILM, often referred to as stellate maculopathy which are better seen on red-free fundus photography
- Peripheral retinal schisis occurs in 50% of cases
- The most common location for this peripheral schisis is the inferotemporal quadrant
- Potential findings at later ages as the condition progresses may include RPE changes. macular hole, retinal dragging with vitreous strands, complicated with vitreous hemorrhage and rhegmatogenous retinal detachment
Ancillary Test
- Fluorescein angiographic reveals similar pattern to that of cystoid macular edema, but without leakage of dye in the late phase
- Visual field testing shows an absolute scotoma that corresponds to the areas of peripheral schisis
- ERG shows refuced photopic and scotopic b-wave
Management
- Observation, since this is a slowly progressive condition where patients maintain their visual acuity for a long period of time
- Surgical management is necessary if complications such as retinal detachment, vitreous hemorrhage or macular hole should occur