Epidemic Keratoconjunctivitis
- The most common cause of "pink eye".
- Self limiting disease.
Clinical Features
- Very acute and highly infectious external eye infection caused by Adenovirus type 8 and 19.
- The spectrum of the disease could be from mild and inapparent, to full blown cases.
- Symptoms:
- Foreign body sensation, photophobia, conjunctival hyperemic, eyelid stuck together in the morning, eyelid edema and sero-fibrinous discharge
- Ocular symptoms commonly preceded by systemic symptoms of fever, sore throat and sometimes gastrointestinal disturbances
Signs
- Acute onset of unilateral, followed by bilateral papillary and follicular reaction
- Bilateral tender and enlarged preauricular lymph node
- Diffuse epithelial punctate keratitis end erosions over the central cornea appear during the first or second week of the disease
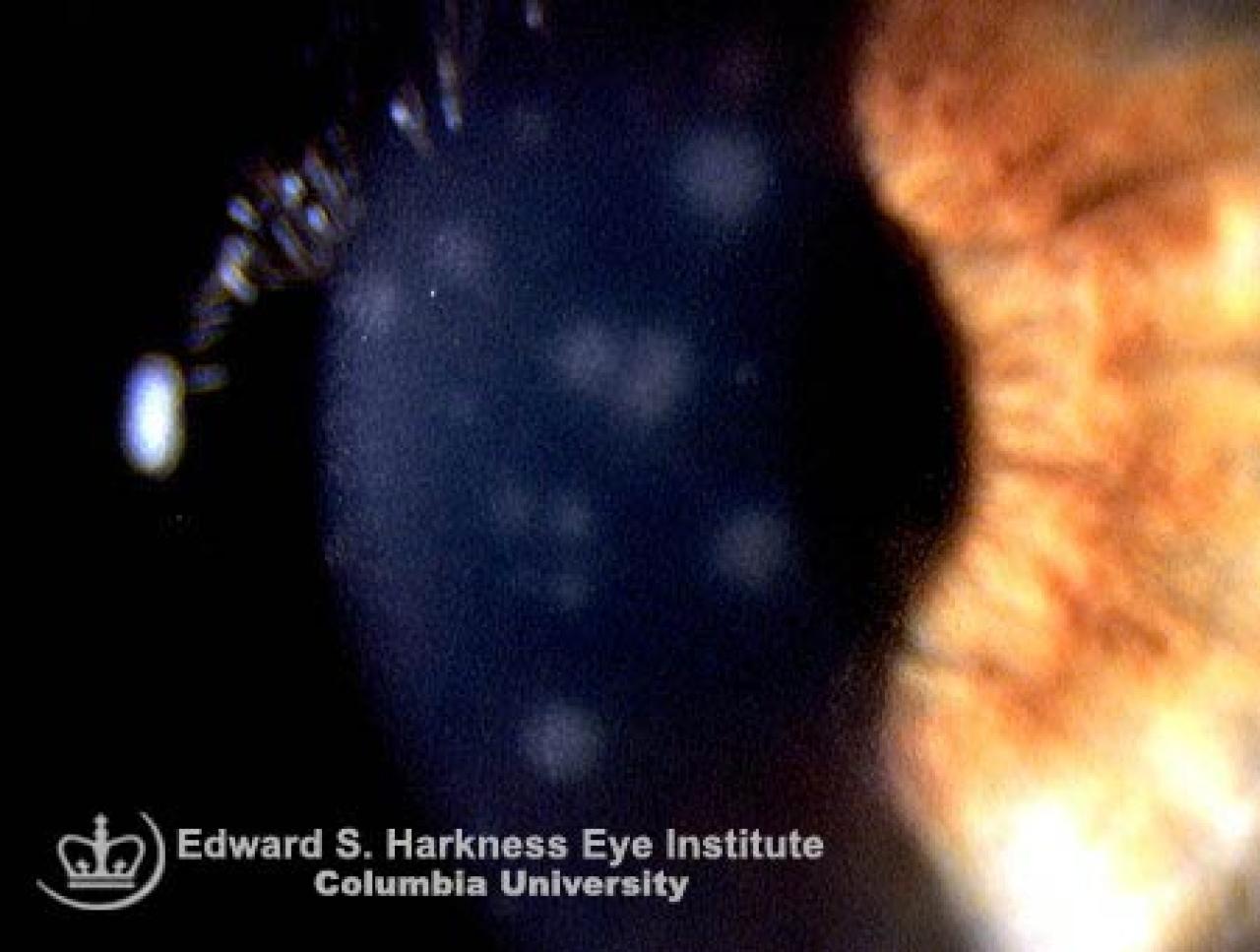
- The epithelial lesions gradually coalesce and form coarse spots of subepithelial infiltrates
- These small-rounded subepithelial opacities may persist for weeks, months or even years
- The first affected eye usually will suffer from relatively more prominent and prolonged keratitis than the fellow eye
- Pseudomembrane formation may occur and can be complicated with conjunctival scarring and symblepharon
- The viruses can be readily spreaded by finger to eye contact, therefore hand washing and proper disinfection of instruments after contact with any patient suspected of having EKC are mandatory.
Management
- Symptomatic relief with artificial tears and systemic analgesic maybe required.
- Topical corticosteroids and cycloplegic are useful in patients with marked iritis and central corneal subepithelial infiltrates